Hello party people! So we’re back to finish up our chat about malaria. Last week I took you behind the scenes with the curious parasite (Plasmodium falciparum) that causes malaria, and its obnoxious insect carrier, with the face for radio, the Anopheles mosquito. Today I want to focus on the disease itself. Sure, having a parasite that rapidly divides in the liver and spreads through the blood stream clearly doesn’t sound as fun as dinner and a movie but how exactly does our body respond to these microscopic freeloaders?
Hello party people! So we’re back to finish up our chat about malaria. Last week I took you behind the scenes with the curious parasite (Plasmodium falciparum) that causes malaria, and its obnoxious insect carrier, with the face for radio, the Anopheles mosquito. Today I want to focus on the disease itself. Sure, having a parasite that rapidly divides in the liver and spreads through the blood stream clearly doesn’t sound as fun as dinner and a movie but how exactly does our body respond to these microscopic freeloaders?
Fun fact – Mosquitos do not depend on blood as their primary food
source. Most of the time they eat like vegan, yoga instructors,
feeding on sap and flower nectar for carbohydrate fuel to power their
airborne lifestyle. Blood becomes a necessary source of protein for
developing eggs. So it is actually the female Anopheles that goes buzz
in the night.
Act I – Incubation stage
 I don’t know about you, but if I just moved into a new apartment I need a few days to get settled in, unpack some boxes, and tape my Marley posters to the wall before I throw a party. Plasmodium falciparum is no different. At this point the Plasmodium is still hanging out in the liver cells. It can take up to 30 days after the
I don’t know about you, but if I just moved into a new apartment I need a few days to get settled in, unpack some boxes, and tape my Marley posters to the wall before I throw a party. Plasmodium falciparum is no different. At this point the Plasmodium is still hanging out in the liver cells. It can take up to 30 days after the
initial infection before the first symptoms appear, and those range in severity.
Act II – Blood stage

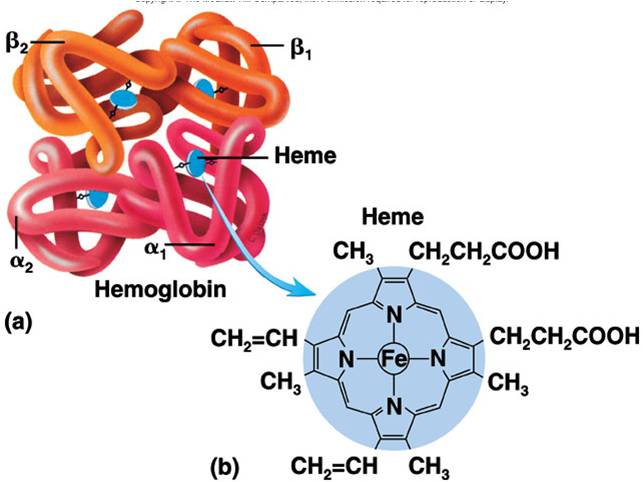
a closer look at the hemoglobin protein. P. falciparum converts the heme subunit to hemozoin.
The chaos ensues once the Plasmodium disperses from the liver and begins circulating in the blood stream. It’s the hemoglobin protein in our blood that they’re after. I don’t want to wander too deep into biochemistry, but if you recall from my earlier article on blood, each hemoglobin protein contains a vital compartment called a heme group. This contains a tiny molecule of iron at its core. This is what binds
the oxygen in our blood. Heme is also toxic when it is released from the hemoglobin. To get around this toxicity the Plasmodium can store heme molecules in their single-celled body in an insoluble, crystallized form called hemozoin. Inevitably the red cells lyse,
releasing the plasmodium along with all the waste products leftover from their hemoglobin feeding frenzy, to include hemozoin. This becomes bad news for us.
When it comes to our immune system our blood stream is a small town
and our white cells hate strangers with a passion. Eventually,
wandering T-cells with the right receptors will encounter Plasmodium
merozoites in the bloodstream (by detecting dsDNA on their membrane
surface) which triggers the release of pro-inflammatory cytokines. However the hemozoin that is released when the red cell ruptures seems to trigger an immune response on its own.
Unfortunately, our immune response is not always strong enough to
completely clear the infection. This is partly due to the many changes
the plasmodium goes through in its life cycle that allows it to dodge
the immune response. It goes through 7 stages, altering its
biochemistry a little each time.
One of the classic presentations of this disease is intermittent
fevers. Typically when your fever stops you start to feel better, but
with a malarial infection fevers often occur in waves every 48-72
hours. This is the result of the rupturing of blood cells as the
parasites continue to multiply and invade new cells.
Signs and Symptoms

That’s right, I know what you really really want…
Think back to the last time you or someone you’re close to had the
flu. When you get hit with the flu you typically look awful, drunk, and exhausted like you haven’t slept since the Spice Girls were last on tour. During classic cases of P. falciparum infections, patients will present with “flu-like” symptoms of high, persistent fever, headaches, chills, sweats, anemia, and vomiting. Remember that during the blood stage of the infection blood cells are being destroyed. So the patient is weak and essentially poorly oxygenated. It is basically a parasite-linked anemia.
Malaria can become deadly if left untreated when infected cells begin to clock capillaries of the brain (cerebral malaria). This can ultimately lead to brain damage, coma, or death.
Testing Methods
We can identify malaria directly from a peripheral blood smear where a
giemsa stain is added to a drop of infected blood on a glass slide and
examined under the microscope. This kind of testing is wonderfully
direct. The problem with poorly developed countries is that proper
testing facilities, microscopic equipment, and trained professionals
who know what to look for are in short supply. So there are RDT’s
(rapid diagnostic tests) available that can identify specific malarial
antigens in patient blood samples. Much like a Strep or flu test, the
patient’s sample is combined with a reagent in a tube or cassette
where a qualitative reaction (positive or negative) can be observed.
However, depending on the concentration of Plasmodium in the blood a
patient may have a false negative. So there is still a need for
confirmatory testing, especially in areas of the world (I’m looking at
you Africa) where drug resistant cases are high.
Treatment
Good Ole Chloroquine…
So we know the plasmodium needs to break down the hemoglobin in order to use those lip-smacking amino-acids while not poisoning themselves with the heme that gets released. So they form hemozoin crystals of the heme to disarm its toxicity.
Welcome to the wonderfully clever world of chloroquine. This drug diffuses into the Plasmodium, halting their ability to form hemozoin crystals. This allows the heme to build up in their nasty little bodies, shutting down their metabolism. Sadly, chloroquine resistant malaria is common place in malarial hot zones. In these cases patients require drug combinations like quinine sulfate and tetracycline.
You also have to manage the mosquito side of the disease. Spraying for mosquitos to control the population has been effective in many urban settings. We also have to understand the behavior of the mosquito. Anopheles prefers to feed at night until the wee hours of the morning. So distributing sleeping nets in malarial hot zones can literally save lives.
The CDC has mapped out malarial zones around the globe. So travelers are encouraged to seek malarial prophylaxis to prevent infections.
Here’s the bad news you already know..
– Children are the most at risk from malaria. In fact it kills more children globally than anything else.
– Diseases thrive in areas where the population is dense and the
availability of adequate healthcare is scarce. This creates a scenario
where the mosquitos are more likely to bite infected individuals. An
infected population left untreated inevitably leads to a more
resistant disease.
Luckily we don’t live in a vacuum and we can contribute. There are a number of organizations out there committed to finding solutions for this global problem. Here’s one organization I happen to like (no, I’m not affiliated with them)
http://www.malarianomore.org/pages/the-challenge
Hopefully I cleared a few things up about this topic. If you have questions please leave me a comment.
As always, stay curious, stay classy, and never stop learning my friends 🙂