
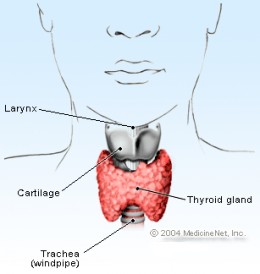
Apparently not even the invisible man can hide his trachea
Metabolism – the way our bodies produce and utilize energy on a cell to cell basis to keep us alive to jazzercize another day is largely regulated by a funky looking, butterfly shaped, hormone secreting gland we affectionately call the thyroid.
Alright people let’s talk about the details…
It would be nice if all we needed to know about the thyroid was that it produces thyroid hormone. Yes, but you’ll never reach academic rock stardom that way so…
What we refer to as thyroid hormone is actually describing two different forms of one hormone, the active and inactive state. Iodine is a principle component of the molecule and the properties of the hormone are greatly altered by the number and arrangement of its iodine molecules. In fact, if you have a severe enough iodine deficiency in your diet you can develop an enlarged thyroid gland called a goiter, which is probably the worst looking hickie you could get without the makeout party ( I wouldn’t know).
When T4 (thyroxine) is secreted by the thyroid gland it circulates through the bloodstream inactive until it can be deiodinized and converted into its active form, T3(triiodothyronine).
Now the hormone is primed and ready to mingle, binding to cell nuclear receptors, initiating RNA transcription, protein synthesis, and kicking ass all over the place, driving our cells to burn energy, oxygen, and be all they can be.
All of this T4/T3 magic is of course made possible by our friend the pituitary gland which produces the trophic hormone TSH (thyroid stimulating hormone) which triggers the production of throid hormone by the thyroid.
In addition to increased metabolism, thyroid hormone also raises the heart rate and respiration. If we are talking about the human engine here, an increase in respiration draws in more oxygen which our bodies utilize to burn more calories. This hormone also triggers the breakdown of glycogen stores in our cells (glycogenolysis) which releases glucose back into the bloodstream making it readily available for energy.
But wait there’s more…
Parathyroid hormone (PTH) and the opposing action of Calcitonin
We’ve only discussed half of this magic butterfly’s mad skillz. There is yet another hormone produced by the thyroid that we affectionately call calcitonin which, along with parathyroid hormone from theparathryroid glands, regulates calcium levels in the blood. HOw? Excellent question…
Your parathyroid glands rest behind the thyroid, and while not getting their hands dirty with metabolic regulation, they are largely responsible for the regulation of calcium levels in the body…which is kind of a big deal.
Our bones are the largest source and sink for calcium in our bodies. So when the pressure is on to get calcium circulating in the blood again our bones play an award winning, supporting role. There are these crazy cells called osteoclasts which are basically differentiated macrophages (white cells of the bone marrow) that specialize in degrading bone. This is regulated largely by the opposing actions of parathyroid hormone and calcitonin.
When more calcium is needed in the blood PTH indirectly stimulates the formation of new osteoclasts from macrophage precursors which degrade bone minerals with the use of acid from their cellular stomachs, lysozymes. How cool is that? (feel free to say “very cool”). The role of PTH is indirect because in its absence osteoclast formation would normally be inhibited. PTH basically plays matchmaker, stimulating osteoblasts (cellular precursor) to produce stimulating factors and express certain membrane receptors. When macrophages come under the influence of these factors (and the mood is right) they differentiate into osteoclasts.

*sigh…doesn’t it make you tear up with after school nostalgia?
These cells differentiate when chemical signals activate their membrane receptors to trigger a physical change within the cell. It’s kind of like when Tommy morphs into the white ranger whenever Zordon calls him on his gigantic 90’s cell phone (do my Power Ranger’s references turn you on ladies?Please, try to focus). When blood calcium levels are just right or too high calcitonin is released, which inhibits the action of those osteoclasts on the bone and basically tells them “nada mas.” This allows for the calcium to be reabsorbed by the bone, reducing the levels of Ca2 in the blood. Calcitonin also inhibits calcium absorption by the intestines as well as the resorption of calcium by the nephrons (tiny functional units of the kidneys) which allows it to be released in the urine when we….um…well..release our urine. PTH, on the other hand, stimulates the absorption of calicium by the intestines and promotes the production of vitamin D through various biochemical means that unfortunately can not be explained with simple Power Rangers analogies.
The actual physiological role of calcitonin is still a tad hazy however, since research has not been able to show significant changes in the regulation of calcium as a result of thyroid tumors or the removal of the thyroid (thyroidectomy).
Thyroid Gland Greatest Hits
increases basal metabolic rate, increasing the rate at which oxygen and energy are consumed
increases the rate of protein synthesis to include RNA polymerase
increases production of Na+/K+ and ATPase – the cell bound molecular generator of ATP(adenosine
triphosphate) that are cells utilize to power numerous enzymatic activities
increases the rate of glycogen breakdown (glycogenolysis) and cholesterol breakdown
increases heart and breathing rate
When Thyroids Attack

sorry, very few pictures of thyroid gland attacks in the wild. Flipper here will have to do
Yeah I know, something always has to go wrong doesn’t it? We just can’t have nice things.
familiarize yourself with these two prefixes – hyper v.s. hypo When you see these prefixes think of more v.s. less, overactive v.s inactive
Let’s face it, any organ or organ system intimately involved in maintaining homeostasis within the body – that zen-like state of metabolic harmony, is susceptible to malfunction. For example, when the thyroid comes under attack by antibodies from the body’s own immune system it can effect it in one of two major ways…cause the overproduction of thyroid hormone (hyperthyroidism) or it can lead to the decrease of activity or rather the ineffectiveness of the thyroid (hypothyroidism). Both conditions can range from either mild to severe with the severe cases named after the clever, tenacious science folks that researched them ergo…Hashimoto’s thyroiditis and Grave’s disease.
General Characteristics of Hypothyroidism (not necessarily associated with autoantibodies)
weight gain associated with decreased metabolic rate
hypoventilation
decreased cardiac output
lethargy
mental slowness
drooping eyelids
goiter
General Characteristics of Hyperthyroidism (not necessarily associated with autoantibodies)
weight loss associated with increased metabolic rate – (which sounds good, but it’s not in that sexy, southbeach diet way)
increased heat
increased cardiac output
tremors
weakness
goiter
Domo Arigato Mr. Hashimoto (Hashimoto’s thyroiditis)
– severe form of hypothyroidism antagonized by autoantibodies directed against the thyroid cells. It most commonly affects middle aged women. Patients exihibit chronic, severe symptoms of hypothyroidism mentioned above.
Grave’s Disease
– severe form of hyperthyroidism antagonized by autoantibodies directed against TSH receptors. This disease is also more prevalent in women. It’s signature characteristics include eye bulging, heat intolerance, nervousness, irritability, and weight loss.
Stay curious, stay classy, and never stop learning my friends
