After two pink bags of cotton candy all the rides were a little blurry that day.
Ok brace yourself, because I’m about to make a painfully obvious statement. Sometimes what we say we’re feeling and what we are actually feeling is not the same thing. Yes, you do it too. Oh yes you do! Do I need to call your mom and let her know your pants are on fire? Listen, I don’t want to fight about this, but I will say that there are a handful of terms good people like you and I use to tell our doctors what we’re feeling because we don’t know any better. For example, when was the last time you felt dizzy? Perhaps I should say lightheaded, or that you felt like you were going to faint (presyncope). Maybe you felt like the room was spinning (vertigo).
We use “Dizzy” to describe all of these sensations when in fact sometimes we’re only experiencing one of them. When the teenager behind the counter at the ice cream shop takes your order you don’t say “give me two scoops of the really cold kind” do you? Sometimes names matter. Well get ready, because we’re about to get technical.

Hey Buddy, maybe you should sit down. You look like you need a juice box.
Light headedness is typically the result of a sudden drop in blood pressure (hypotension). Our bodies are a lot like one of those giant, dancing balloon characters outside of a used auto dealership. You cut off the fan (the air flow) and the balloon man falls to the ground. Well when our fan shuts off (our blood flow to the head is restricted) we faint. We refer to this as “syncope.” That feeling that we are about to faint is “presyncope.” We can also experience the lightheaded blues when we stand up too fast and we refer to this as “orthostatic hypotension,” where the blood flow is affected by the positioning of the body. Ok blah blah…that’s all very interesting (yawn), but I want to get to the good part, vertigo.
Vertigo is CRAZY interesting. Actually, for the rest of this article I’m just going to talk about vertigo. Everything else is dead to me.
Vertigo is a profound sensation of disorientation. You can have the feeling that the room is spinning or that you are spinning. You can also experience the sensation of falling or that the ground or room is tilting. All of these trippy sensations can make you feel incredibly off balance and often lead to nausea.
All of these sensations are caused by a malfunction (minor or severe) in the way your brain is receiving information from the balance organs of the body. What kind of malfunctions you ask? Well if the possible causes of vertigo were a dusty road in New Mexico that split in two, one road sign would read “sensory neural pathway” and the other would read “organs of the inner ear.” Need more? As the comedian Bernie Mac used to say, “Let me break it down for you like a fraction.”
Your brain talks to your body constantly. Like an overprotective mother the brain asks your eyes “where are you? What are you doing right now? What do you see?” However, Mother is just looking out for us, taking that visual input and coordinating our skeletal muscles/motor control to maintain an upright posture and orient the fluid within our inner ear like the bubble in a carpenter’s level (see fig. 2) so that we have an accurate perception of up and down, left and right, backwards and forwards. That intimate communication between brain, eyes, and motor control is referred to as the vestibulo-ocular reflex. Go ahead and click this link
https://forgottenphysiology.com/2013/12/19/me-talk-pretty-vestibulo-ocular-reflex/
it won’t bite 🙂
Balance is in your ears?
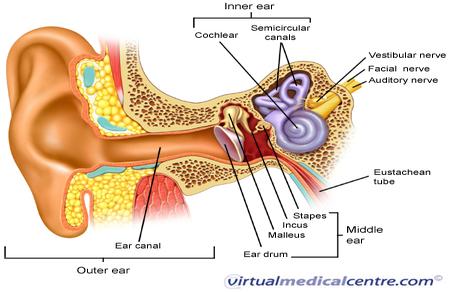
This balancing act is brought to you by our inner ear. The physical interaction of sound waves within the intricate, spiraled canal of bone called the cochlea in conjunction with the stimulation of auditory nerves are largely responsible for how we hear sound. However, one of the more mystifying tricks our inner ear can perform is that of our perception of balance. Alright, we need to zoom in on this thing. Look down there…

ok keep your eyes on the swirlie, looping purple thing (labyrinth of the inner ear) in the diagram. This is where the magic happens.
No no, I mean closer than that…
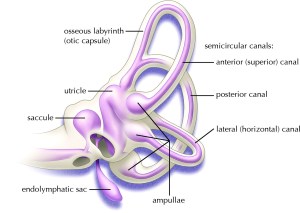
Welcome to the Labyrinth of the inner Ear

A special thanks to Thing for demonstrating the Carpenter’s level
This structure has more twists and turns than a back road in Lexington, Virginia so I’m only focusing on two main parts for now, the semicircular canal and the otoliths. That reminds me, how familiar are you with building houses? That’s ok, just look to the right of the screen. See that’s a carpenter’s level. Builders set it on top of fence posts, center blocks, steel support beams and anything else they need to have level with the ground. That bubble in the center tells them how far off they are. Inside each ear are three very similar structures, semicircular canals, made from bone and tissue that your brain communicates with to maintain rotational balance and orientation (like when you’re busy doing back flips like Night Crawler from X-men). These are tiny, fluid filled canals that loop parallel and perpendicular to each other. That itty bitty amount of fluid inside pushes on the hairs of a structure called a cupula that translates that mechanical movement of the fluid into an electrical message that tells the brain something like “hey, this guy’s doing a cartwheel.” You have three of these in each ear; anterior, posterior, and horizontal that correspond to vertical, horizontal, and diagonal rotations of the body.
The more you learn about the structures of the inner ear the more this all begins to sound like some freaky game of pinball, but we’re not done. The otolithic organs allow us to sense linear acceleration by aid of tiny crystals suspended in viscous fluid [I always thought the term viscous was kind of creepy, but that’s just me]. We have two otolithic organs on each side; the urticle, and the saccule. The urticle is tuned-in to horizontal movement and the saccule is all about the verticle changes in position.
The otolith organ is this crazy looking sac of fluid with a cluster of sensitive hairs. The fluid as I mentioned before is thick, viscous and contains a lot of tiny calcium carbonate crystals that make it grainy as well. So when the head moves this nasty substance produces friction against the hairs and that inertia is translated into vertical and horizontal linear movement by the brain.
Back to Vertigo
When you are suffering from vertigo disruption of the balance organs (especially those of the inner ear) and the sensory neural pathways that talk to those organs are typically suspected. Benign paroxysmal positional vertigo (BPPV) is common when there is inflammation from infections or injections. If inflammation is significant enough it can disrupt the movement of otolith crystals within the inner ear, sending mixed signals to the brain. That can definitely make you feel like you went too many seconds on the mechanical bull in Salt Lake City.

Brother, what a night it really was…
Stay curious, stay classy, and never stop learning my friends 🙂

 Known on the streets as the withdrawal reflex, NFR refers to our body’s involuntary, ninja-quick neuromuscular response to pain. It’s our super sexy physiology term of the week and quite possibly our spiciest one yet. I even like saying it out loud (sometimes in a French accent).
Known on the streets as the withdrawal reflex, NFR refers to our body’s involuntary, ninja-quick neuromuscular response to pain. It’s our super sexy physiology term of the week and quite possibly our spiciest one yet. I even like saying it out loud (sometimes in a French accent).